|
Home | Search | Browse | About IPO | Staff | Links |
|
Home | Search | Browse | About IPO | Staff | Links |
|
By ANTHONY MAN State's Madicaid funding, or fingers in the dike Faced with the choice of balancing the state budget on the backs of the poor, cutting education and other popular programs, or a general tax increase, the legislature and governor selected a fourth option: balancing the budget on the back of the federal government. If the somewhat tenuous scheme holds together, it would result in vast improvements in funding for Medicaid, the program that pays for health care for the poor and constitutes one of the biggest and fastest growing areas of state spending. The advance would be achieved through a system that is simple, at least on the surface. The state has seized on the federal government's practice of matching state spending on Medicaid. In Illinois' case, the federal government reimburses the state $1 for every $2 of spending. To capture more federal money without raising general taxes or cutting spending, the state imposed a tax on hospitals, nursing homes, and centers for the mentally ill and developmentally disabled. The tax on providers is levied on their Medicaid income. The money raised isused to snare matching funds from the federal government, and the new, higher pool of funds is available for the state to pay its bills for Medicaid services provided by the same entities that paid the special tax. Everyone seems like a winner: Medical providers, who have been chronically underfunded by the state, get more money; health priorities get a little more attention because there is new money available to spread around; and, of course, every other state function benefits because money from the general revenue funds is freed to be spent elsewhere. "It's a gain for everyone. It's a gain for the state and it's a gain for every Medicaid provider in the state," said Sen. Penny L. Severns (D-51, Decatur), who sponsored an earlier version of the provider tax limited to hospitals. The provider tax was so good, for Illinois, at least, that it passed the House and Senate unanimously and quickly got Gov. Jim Edgar's signature. (The massive tax increase got curiously little attention. The Edgar administration insisted the governor did not break the emphatic no-new-taxes-for-four-years pledge he made during last fall's campaign. Gubernatorial spokesman Mike Lawrence said this was not an ordinary tax because those who pay get it all back.) The federal government, however, regards Illinois-type provider tax systems as fraudulent raids on the U.S. treasury. From a policy standpoint, mechanisms like the hospital-nursing home tax are not seen as genuine state contributions deserving of a federal match. Practically, these efforts are becoming enormously expensive for the federal government. A memorandum from the inspector general of the U.S.Department of Health and Human Services recommended changing the rules and laws that allow the Illinois-type provider tax systems. "Conceivably the federal government could ultimately be required to bear a disproportionate share of the entire cost of the Medicaid program unless the 'loopholes' are closed," the memo states. "The growth of provider tax and donation programs is almost like an uncontrollable virus spreading from state to state." Philip C. Bradley, director of the Illinois Department of Public
August & September 1991/Illinois Issues/33
Aid, sees a certain kind of justice in the states' moves to shift some Medicaid costs back to the federal government, which has been greatly expanding the number of recipients and the benefits for which they are eligible in recent years. States must pay for part of the expansion, which is one reason they are having trouble coming up with their shares. To some extent, this is retribution for all the new federal mandates. There are conflicting theories about whether these provider tax programs by the states will be stopped by the federal government. Those who believe they will be permitted to continue think the growing number of states utilizing the approach will provide a critical political mass that will make repeal impossible. One factor in favor is Republican governors, such as Edgar, who are balancing their budgets with federal Medicaid money. Another advantage is that key members of Congress presumably will side with the states. Illinois officials have already enlisted the state's clout-heavy congressional delegation, which includes House Ways and Means Committee Chairman Dan Rostenkowski (D-8, Chicago), House Minority Leader Bob Michel (R-18, Peoria) and the reelection-seeking U.S. Sen. Alan J. Dixon (D, Ill.), always happy to be seen as helping the home state. The contrary view holds that the growing popularity among the states ultimately makes these provider tax programs so big that they will sink of their own weight. One estimate of the cost to the federal government is an unexpected $4.5 billion a year. Under the five-year budget agreement struck last year in Washington, domestic spending increases must be offset with reductions in other areas. So, while Bradley said he did not "think Illinois and other states that have a stake in this are easy to ignore," and Edgar vowed "quite a battle," the outlook is uncertain. "This might go away after six months, this might go away after a year, or it might last permanently," Bradley said. The Illinois law has no general sunset, although the provider tax on hospitals is set to last only four years. Even most pessimists figure the mechanism is safe at least until January. Assuming it remains in place, the hospital and nursing home industries will be much better off. The taxes on medical providers would bring in an estimated $640 million in the current fiscal year, making the total generated by provider tax and federal contributions $1.3 billion in the first year. (While legislators appropriated $1.3 billion from the provider tax and federal match it will leverage, the administering Department of Public Aid said it would not all be spent by the June 30,1992, end of the fiscal year.)
34/August & September 1991/Illinois Issues
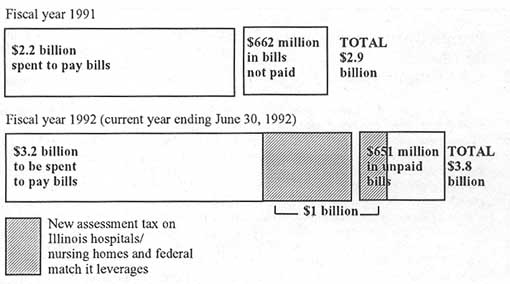
When the $1.3 billion is combined with existing Medicaid spending, medical providers and the people they serve would see significant changes. Beneficiaries would include: •Disproportionate-share hospitals. Those facilities care for an unusually high share of Medicaid patients. Chronic government underpayments on a large caseload makes their finances more precarious than most hospitals'. The provider tax and matching federal money would allow full funding of an existing state program of special payments designed to get them more money. • Costly but vital services. Trauma care for emergencies and obstetric services at hospitals performing a large number of deliveries would be eligible for special access payments. Money is aimed at those services because they are considered important by policymakers and they are often financial drains on hospitals. The idea is to help prevent the shutdown of those critical services for everyone, but particularly in areas with a high Medicaid population. • Advocates of financial incentives to improve quality. The hospital payment mechanism is being revamped, and the Quality Incentive Program for nursing homes is being updated and getting more money. (See the accompanying boxes on reforms in the way Medicaid pays hospitals and nursing homes.) • Cook County Hospital, which will have its own fund similar to those for other providers. Because its Medicaid and uncompensated care loads are so heavy, Bradley said the provider tax system means Cook County Hospital would get another $134 million from the federal government. Also, special Illinois Department of Public Aid staffers would be placed at the hospital to ensure that all eligible people are enrolled in Medicaid. This is designed to ensure that as much money as possible is captured from the federal government and to minimize the amount of uncompensated care. Bradley said there are even more general, widespread benefits from the added money. "If you have adequate money in the system, you have a more reasonable expectation that you'll get better care." He said the biggest winners are poor people in Chicago who are less likely to suffer additional hospital closings. The director concedes that more closings were almost guaranteed under the original budget proposed for his agency. Also benefiting, Bradley said, would be the people who depend on the state to cover their nursing home bills. Medicaid pays for the majority of nursing home residents in Illinois, typically middle-class people whose savings were drained by the high costs of long-term care. Although nursing home troubles do not generate the publicity of a hospital closing, William L. Kempiners said low payments are financially ruining some of his nursing home association's members and forcing some to change ownership. Kempiners, a former legislator, is executive director of the Illinois Health Care Association. An American Hospital Association study released in June found Illinois was worst in the nation in paying for Medicaid patients. Illinois paid on average 53 cents for each $1 it cost to provide service to a hospitalized Medicaid patient; the national average in 1989 was 78 cents. It has been so long since the state performed a nursing home cost study that Kempiners said similar numbers are not available for his industry. Neither Bradley nor executives in the associations representing hospitals and nursing homes could estimate just how much better they would fare under the new provider tax system because payment rules are still being drafted. "A lot of things August & September 1991/Illinois Issues/35 [can] happen in the rule-making process, and I don't know that anyone can truly calculate what the average is going to be," said Adrienne M. Levatino, an Illinois Hospital Association vice president. Any higher payment level provides another kind of benefit that is indirect and hard for most people to see. Currently, hospitals cope with low government payments by shirting the cost to private-paying and insured patients. That helps drive up the cost of health insurance. The Illinois Hospital Association has said that if Medicaid covered all its costs, the bills for everyone else would decrease. This would not necessarily change the total amount spent on health care in Illinois, but each party supposedly would be covering its fair share. Medicaid's problems will not go away with this legislation, however. For one thing, the state's financial problems mean that institutions will wait a long time before they actually get cash, even though the money is budgeted and theoretically available. Despite the Edgar administration's assertion that the budget makes enormous headway in paying off "old bills," figures from the Department of Public Aid show there will be plenty of new "old bills" at the end of the fiscal year on June 30, 1992. (See accompanying chart.) Besides the political advantages from the peacefully negotiated settlement, the state had another incentive to act. Both industries are suing the state on the grounds that payments are so low they violate federal law. (See "Hospital lawsuits challenge Medicaid system in court," Illinois Issues, February 1991.) The hospital association agreed to drop its case as part of this deal. The nursing home industry, however, was unwilling to entertain Bradley's request. "No way," Kempiners said. Federal law requires payments sufficient to compensate an economically run nursing home, and operators figure a victory could give them an even better long-term chance at higher payments. Although the associations representing nursing homes signed off on the provider tax system, Kempiners said it is not a long-term solution. "I basically see it as a bridge. It's a mechanism to hold us together as an industry until such time as a more solid solution comes along." A court ruling in favor of the nursing homes could be particularly important if the provider tax plan falls apart. The law includes a clause automatically cutting rates to the level proposed in the governor's original March budget proposal. Those rates were lower than the amounts paid last year. That could mean financial disaster for the hospitals and nursing homes that agreed to the provider tax plan. No one knows what would happen if the federal government stops the plan. Speaking to reporters at the end of the overtime legislative session, the chief Senate budget negotiator, Sen. Howard W. Carroll (D-1, Chicago), admitted as much: "There is no fallback." Anthony Man is Statehouse bureau chief for the four Lee Enterprise Inc. newspapers in Illinois. He writes frequently about health care issues 36/ August & September 1991/Illinois Issues |
|
|