|
Home | Search | Browse | About IPO | Staff | Links |
|
Home | Search | Browse | About IPO | Staff | Links |
|
By GRACE KAMINKOWITZ
Welfare and medical assistance
leveraging federal dollars for state programs Twenty-two years ago, facing a daunting fiscal crisis, Gov. Richard B. Ogilvie began his administration by securing Illinois' first income tax. Two years later it was clear the state's fiscal problems had not been solved, in part because of mounting welfare costs. By the time his term was up, Ogilvie and his coterie of bright young assistants had pulled off a massive raid on the U.S. treasury, winning hundreds of millions of dollars to pay for federally mandated state programs. In an analysis of how Illinois pried open the federal coffers, Martha Derthick wrote for The Brookings Institution that Ogilvie "identified the welfare crisis of 1972 as 'the climactic issue,' which he had dealt with by cutting general assistance costs and getting large federal commitments on several front." "Illinois made up its budget deficit," she said, "with federal funds" from what was then the Department of Health, Education and Welfare (HEW). She concluded, "While there was pride and satisfaction in Illinois, there was neither in HEW. The department's policy on social services was a shambles, and spending was out of control altogether." Two decades later, Gov. Jim Edgar has faced similar budget crises, also largely because of rising welfare costs. So far, with the perverse help of a Democratic-controlled General Assembly determined to play one-upmanship with the Republican governor, Edgar has managed to keep his campaign promise to hold the line on further income tax increases beyond the .5 percent surtax in effect since July 1989. Like Ogilvie, he has led a raid on the federal treasury to help him hold the line, especially to finance the Medicaid program. There is a big difference between the two administrations. Although the Edgar administration has drawn down its financial commitment to its poorest residents, it has tried to compensate by making its welfare programs more productive. The Illinois Department of Public Aid (DPA) oversees Medicaid as well as other welfare programs that provide social services and income assistance to those who qualify. Public Aid Director Phil Bradley sits in the catbird seat, administering the programs that provide services to approximately 1.6 million Illinois residents. He says, "We serve an enormous number of people, and they're not a homogeneous group. Today we're taking a more sophisticated approach of tailoring our programs to our different populations. We're putting our money where it will do the most good helping people get back on their feet." Instead of the broad-based programs of the past, Bradley's philosophy is to invest in targeted preventive action. Second only to education in the size of its appropriation, DPA's fiscal year 1993 funding was $6.4 billion. Although the average person tends to think that all those dollars are disbursed to welfare clients, the reality is much more startling: For every dollar provided in income assistance, $4.34 is paid to health care providers, mainly reimbursing hospitals, nursing homes, physicians and laboratories. In the light of the disrepute in which the public generally views welfare programs, it is less surprising that the state has severely limited its commitment to the poor when it has to use only its own scarce tax dollars. The state has deliberately pursued a policy of moving away from programs that have no federal dollars to leverage. Add to that the fact that no one appears satisfied with the state of welfare programs. Too many are on welfare; too few are being served. Those providing services complain that the state is either too niggardly in paying the costs of those services or unconscionably late in paying for services rendered. For those getting direct assistance with a check from DPA, the cry rises about once a generation to tie assistance to "work" or some form of job training. And always there is suspicion of welfare fraud by individuals or service providers. Programs come. Programs go. Sometimes it appears that programs are created with merely the expectation that they'll be successful; if they're not, others take their place with the hope that someday something will work. Currently Phil Bradley and the Edgar administration are touting Healthy Moms/Healthy Kids and Earnfare, both passed by the General Assembly for the first time last June. In February, they announced another package of welfare reform incentives, "Fresh Start," designed to keep recipients in school, help them find jobs and get off public aid. Projected at $3.6 million, the Fresh Start programs will qualify for federal matching funds if authorized by the General Assembly because they have been approved by the U.S. Department of Health and Human Services under the Clinton administration. The package is noteworthy because it breaks dramatically with past "one size fits all" programs: It encourages two-parent families to stay together and to find work without losing benefits; boosts part-time or temporary employment without losing benefits; helps employed homeless families retain more of their income so they can find affordable housing; and gives young noncustodial fathers a chance for education, training and parenting skills. The most clear
March 1993/Illinois Issues/19 indication of Bradley's investment in prevention is the program to assist inner city youths at risk of dropping out of school because of early parenthood. The program aims to prevent long-term welfare dependency by providing job training and counseling on drug abuse, pregnancy prevention, self-esteem and self-sufficiency.
"Welfare" is complex and expensive for government. The medical component is the most expensive. The cost of health care has doubled in the last decade. Expenditures for Illinois' Medicaid program have risen even higher, 64 percent over the same decade. At the same time, the percentage of the needy receiving these medical services has decreased. In the mid-1970s, medical assistance was available through DPA to about 65 percent of Illinois' poor. Today that percentage has dropped to 40 percent, according to DPA, which estimates that as many as 1.2 million Illinois residents neither qualify for its medical programs nor have any other health care coverage. Health care is a priority of the Clinton administration. Inextricably linked to its ultimate proposals are federal reimbursements for state Medicaid programs and other federally mandated welfare programs. While all await the Clinton administration recommendations, Illinois faces the decision this spring on whether to renew the tax assessment of its hospitals and other health care providers, including the so-called "granny tax" on nursing homes. Without those revenue sources, which the Edgar administration has used to leverage greater federal Medicaid reimbursement, Illinois' Medicaid program would have to be curtailed drastically or funded much more heavily by the state's general revenues. It was Bradley and his brain trust, including Theresa Stoica, director of medical programs, who first developed the means of exploiting the federal provision that boosted Illinois' Medicaid funding from the feds. Agreed to by the General Assembly in the last days of the 1991 marathon session, Illinois hospitals and other Medicaid providers were assessed fees based on the Medicaid service. Those fees leveraged greater federal reimbursement, while Illinois' providers of Medicaid services were guaranteed that for every dollar they paid in the assessment they would receive two dollars back. The program permitted increases in reimbursement rates to those providing services to Medicaid-eligible clients in Illinois, greatly improving the financial health of hospitals that were at serious risk of going under. (See Illinois Issues, August/September 1991, pages 33-36.) Almost as soon as the federal government learned about it, President Bush's budget director, Richard Darman, called it a scam. It also was denounced by Gail Wilensky, then the administrator of the Health Care Financing Administration. The Bush people considered it a loophole in federal law that permitted an assault on the treasury and moved with alacrity to close it. The Edgar administration saw it as a salvation for the state budget. Edgar moved that summer to marshal support among members of the National Governors Association and the Illinois congressional delegation. By November 1991, with most other states moving to use the assessment program to trigger greater federal Medicaid funds, a compromise was negotiated with the Bush administration and Congress. The resulting Medicaid Voluntary Contribution and Provider-specific Tax Amendments of 1991 used these major criteria for state participation:
The changes required the General Assembly to pass a revised program last spring or lose Illinois' eligibility on September 30. It was a tough sell for Bradley and Edgar since all hospitals and other medical providers had to be assessed. Wealthier hospitals, especially those in Chicago's suburbs, serve a relatively low number of Medicaid patients. Inner city facilities such as Mount Sinai, Michael Reese and the University of Chicago hospitals serve a disproportionate share of the medically indigent. The redistributive formula obviously meant that the healthier, wealthier hospitals would be subsidizing poor facilities. The Illinois Hospital Association fought passage although its members serving disproportionate numbers of the poor strongly supported the formula. The new plan was passed, but with only one year's authorization, which puts the issue back in the General Assembly this spring. (See Illinois Issues, August/September 1992, pages 18-20.) Specifically, hospitals are assessed at a rate of 2.5 percent of their adjusted gross income. Intermediate care facilities for the developmentally disabled are assessed at 13 percent of their adjusted revenues for services to
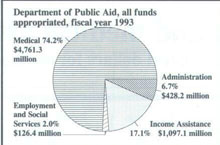
20/March 1993/Illinois Issues their special population. Nursing homes are assessed $6.30 per patient per day. Suburban legislators promptly labelled the nursing home assessment a "granny tax," predicting the facilities would pass it along to their patients. They did. Meanwhile, to protect the most vulnerable nursing home clients who were not on Medicaid but could ill-afford the tax, the General Assembly included a grant program permitting non-Medicaid long-term care patients to apply for a rebate of the $6.30 tax when paying their state income tax. There would be a "means test" with the refunds or grants limited to private-pay patients with annual incomes of less than $53,000. As the General Assembly begins its 1993 budget deliberations, including the fate of the Medicaid assessment plan, the Senate is in the hands of Republicans. But that may be faint help for Edgar whose major opponents to the assessments last session were legislators from DuPage County. House Minority Leader Lee A. Daniels (R-46, Elmhurst) was strongly opposed to the plan and is adamantly opposed to extending the nursing home tax. New federal regulations may require any renewed program to reduce the tax on facilities for developmentally disabled clients, thus lowering revenues by about $22 million which would have to be replaced from general revenue funds. A preliminary report in late January by a subcommittee of the Health Care Task Force, appointed last year, recommended the extension of the Medicaid assessment on hospitals, nursing homes and other providers for two years. The 36-member task force was appointed by Edgar to study the immediate problem and the longer-term issues of cost and access to health care for the state's poor residents. (See Illinois Issues, August/September 1992, page 20, and January 1993, page 29.) Task Force Chair Ernest R. Wish said the committee recommended a two-year extension to provide President Clinton time to develop a comprehensive health care plan for the entire nation. The recommendation also provides cover for Gov. Edgar who needn't face raising the income tax before his expected 1994 election bid. Wish, the retired managing partner of the Chicago office of Coopers & Lybrand, accounting and consulting firm, said the task force also suggested excluding rural hospitals from the tax and that the nursing home assessment be levied at a percentage of their revenues instead of the flat $6.30 fee. It rules out both spending cuts and revenue increases via raising "sin" taxes on alcohol and/or tobacco. DPA has little discretion in its spending because of federal mandates to the states for providing services under national programs administered by the state, especially Medicaid. Only $174 million of DPA's current appropriation from general revenue funds is for nonfederal programs. About $37 million is allocated for administrative costs; the other $137 million is distributed to clients for Transitional Assistance, the remnant of the former General Assistance program without a federal component which Edgar pared to the bone. DPA categorizes expenditures by dividing its fiscal 1993 cash flow into three groups: 1) social services and administration at $478.1 million; 2) income assistance at $1,041.6 billion; 3) and medical assistance (Medicaid) at $4,398 billion. (This adds up to less than the $6.4 billion appropriated because the larger amount includes an extra quarter of assessment funds.) The first category covers employee salaries, overhead plus Project Chance which includes payments to day care, homeless and domestic violence shelters. The second category, income assistance, is what the public generally considers "welfare" and includes payments through Aid to Families with Dependent Children at about $900 million; Aid to the Aged, Blind and Disabled about $66 million; Transitional Assistance about $44 million; Family and Children Assistance about $18 million; and miscellaneous expenses for funerals and burials, refugees and emergency assistance about $10 million. Spending for income assistance has been relatively steady during the last 10 years. Starting at $1,116.9 billion in 1984, it reached a high of $1,176 billion in 1986. It is now down to $1,041.6 billion, a decline of 6 percent over the decade. In February two Washington-based policy groups ranked Illinois among the three states that had most severely cut programs affecting the poor in 1992. One of the cuts cited was the discontinuation of General Assistance which had provided aid to 66,000 single or childless able-bodied recipients considered employable. Medical assistance, the third category, is the behemoth of DPA spending, rising 64 percent in 10 years: from $1,566.3 billion in fiscal 1984 to $4,398 billion in fiscal 1993. The agency's total expenditures during the same period increased 49 percent, from $2,982.9 billion to $5,917.7 billion. Ask DPA Director Bradley for his reasons for Illinois' public aid crisis, and he sounds as frustrated as a city mayor upset with Illinois state government. "Illinois is in worse shape than many states because of mandates," he says. "The federal government mandates that you spend another dollar but they give you only 50 cents. There are states that get 75 cents in federal money for every quarter they spend on Medicaid. The impact on them is less severe from federal government mandates than states like Illinois that get a 50 cent match." Illinois is considered a wealthy state, based on its per capita income, so its Medicaid matching funds come in at the lowest level. Over the years, Congress has changed the programs. In 1981, the Reagan administration sought and got cutbacks in federal assistance. Large numbers were dropped from Medicaid coverage when the administration declared them ineligible for Aid to Families with Dependent Children, but later many came back on the rolls when Congress broadened Medicaid coverage, most notably to include low-income pregnant women, infants and children. In Illinois, that Medicaid-eligible coverage includes one in every two children in Chicago, one in every three births in Illinois and two of every three days of care provided in Illinois nursing homes. In addition, almost 100,000 elderly Illinoisans
March 1993/Illinois Issues/21 have their Medicare insurance premiums paid for by Medicaid. Generally, the services which the state must provide according to federal mandates for Medicaid include inpatient and outpatient hospital services; laboratory and x-ray services; nursing facility services for those 21 and older; physician's services; a nurse-midwife's services; and those of a certified pediatric nurse-practitioner or certified family nurse-practitioner. Also on the must list are prenatal care for pregnant women; ambulatory services for clients under 18 and for those entitled to institutional services; and home health services for anyone entitled to nursing facility services. While medical care costs are DPA's pressing problem, its other programs are often criticized as dead ends, offering little incentive for work instead of welfare. With the laudable goal of breaking the "welfare cycle" for recipients of Aid to Families with Dependent Children, the DPA under the James R. Thompson administration established Project Chance, with mixed results (see Illinois Issues, August/September 1989, pages 52-53). Funded in partnership with the federal JOBS program, Project Chance seeks to train recipients to reenter the workforce. The program was begun in 1986 with the goal of moving 100,000 recipients into paid employment in three years. Although DPA more than met that goal, the positions often were minimum wage and short term. Welfare advocacy groups criticized the program, and Congress made changes through the Family Support Act. The General Assembly's revisions in the program resulted in more emphasis on developing skills for trainees that would enable them to move beyond unstable, minimum wage employment. It also funded the program so that caseworkers were able to lower their caseload from 350 to 100. As of December 1992 DPA says that 241,447 participants in Project Chance since fiscal year 1986 reported that they had found employment after leaving the program. The department does not track what happens to participants after finding their first jobs. Currently there are about 18,000 people in the program, and more are on a waiting list because the legislature appropriated enough for only the 18,000. In fiscal 1992, 11,051 participants moved from Project Chance into jobs. Bradley pushed last year to transform the program or at least a pilot test phase so that it wouldn't duplicate similar programs delivered elsewhere. A longtime trustee of Lincoln Land Community College in Springfield, he realized that DPA was doing many of the things community colleges do. Rather than DPA's continuing the training redundancy, he proposed a test project he calls Opportunities with 10 community colleges (including one in Chicago) that places DPA clients at the community colleges for job training through the federal JOBS program. That permits the DPA to leverage additional funds of about $2.8 million. The test program with the community colleges is scheduled to continue for another year. Bradley is also pushing the new Earnfare program. With its implementation beginning in October, the program matches subsidized jobs from participating organizations across the state to able-bodied out-of-work adults on transitional assistance (see Illinois Issues, August/September 1992, pages 36-38). Funded for fiscal 1993 at $10 million with only state money (no federal funding), Earnfare offers grants for part-time jobs to private, nonprofit, community and government employers agreeing to recruit and train people on transitional assistance for six months. The theory is that the unemployed would in six months gain sufficient workplace experience to enhance their ability to find and maintain permanent jobs. Initially cautious about the program, Edgar has become enthusiastic and plans to recommend increased funding for fiscal 1994. As of February, 5,272 people (4,252 in Chicago) had Earnfare jobs at 337 employers, exceeding the DPA target of 5,000. Some 100 have left the program before completing it because they had found employment. Realistically, Bradley knows that if health care costs don't slow their upward zoom, neither shifting to federal matching funds nor economies with other programs will come up with enough money in the long run to fund medical coverage for the poor. Yet, he believes one new
22/March 1993/Illinois Issues program will serve as a means to reduce long-term costs. It is Healthy Moms/Healthy Kids, his commitment to investing in preventive health care. This program, Bradley explains, is a managed care initiative offering Medicaid-eligible children and pregnant women access to preventive and primary health care. "The program is designed to increase access, to enhance primary care, to eliminate late night visits to emergency rooms which are very costly, and to improve the health of the kids particularly in the city of Chicago," Bradley says. Another goal of the program is to reduce Illinois' embarrassingly high infant mortality rates. "Part of Healthy Moms/Healthy Kids is doing health screenings that the federal government has mandated that we do," Bradley explains. "We develop treatment schedules and see that they're adhered to through active case management. Those treatment schedules will include immunizations," he says, which save funds in the long run. He tells of a measles outbreak in Dallas which cost taxpayers about $5 million. If the children had been immunized, he says it would have cost taxpayers less than $200,000. Under Healthy Moms/Healthy Kids, which is scheduled to begin in April, clients will be able to choose one of five managed care organizations and will be locked into that choice for one year. Physicians will receive rate increases for preventive and primary services plus a monthly managed care fee for each client in an attempt to entice doctors back to serving the poor. A number of hospitals are helping recruit physicians with staff privileges. (Low and slow payment in the past turned physicians away from treating Medicaid clients.) DPA has contracted with First Health Services Corporation, one of the largest providers of computerized case management in the nation, to track program participants and their treatment schedules. In Chicago, the computer will combine DPA and the city's Department of Health systems so that physicians will be able to deal with a single entity. Downstate services will be provided through local health departments and schools. Bradley estimates it will take as long as one year to phase in all the nearly 400,000 clients eligible for the program. Initially funded in fiscal 1993 for $19 million, the program was emphasized by Gov. Edgar in his State of the State address in January. DPA has requested annualized funding for fiscal 1994 of $100 million. Bradley is frankly frustrated with making public policy in Illinois, even policy designed to enhance chances that a child will survive into adulthood. He describes a Chicago hospital maternity ward where the nurse pointed out a baby that had been there for 60 days. She told him the infant was now ready to leave but that he was a Department of Children and Family Services ward, and that the agency had not found a foster home for the baby yet so he remained there with the bills paid by DPA. Bradley also tells about pregnant women reporting to hospitals to deliver their babies, having never seen physicians during their pregnancies. Many are active alcohol and drug abusers who deliver babies weighing one and one-half pounds who need to be hooked up to life support systems. The care of these infants costs DPA $60,000 a week. Bradley hopes Healthy Moms/Healthy Kids will provide the preventive care that will maximize the chances for delivery of full-term healthy infants. Illinois has tried other innovations. In one attempt to hold down its Medicaid spending, the state attempted to limit the increase in costs to no more than the rate of inflation for the economy. Called ICARE (Illinois Comprehensive Access and Reimbursement Equity), the program was dropped in fiscal 1991. While in force, hospitals bid competitively to provide care to Medicaid-eligible individuals, and clients were required to obtain care only from ICARE hospitals. Although it kept Medicaid spending down, health care providers hated it. The low fees and slowness of payment allegedly drove financially troubled institutions out of business. Bradley also explains that DPA has replaced a state-funded program providing medical benefits for adults ineligible for assistance under other programs with one where hospitals can provide this care and receive Medicaid reimbursement. That means an uncompensated care add-on to the hospital reimbursement rate, an option permitted under Medicaid. Now the state receives federal funds for these services formerly paid 100 percent with state funds. In fiscal 1992 DPA claimed $17 million in federal Medicaid reimbursement for these services; the amount for fiscal 1993 is expected to be about $30 million. A smaller program deals with a vaccine replacement plan implemented by DPA. Formerly funded by the state's federal Title XX Social Services Block Grant allocation, Bradley shifted the costs to Medicaid to received a 50 percent federal reimbursement of $2.2 million, thus freeing those Title XX funds for other social services. Bradley also is pursuing "enhanced funding" for a food stamp fraud unit that goes after stores and systemic fraud. The federal government will pay 75 percent which translates into $1.2 million for the state's coffers. Illinois also will be permitted to retain 25 percent of all food stamps recoupments resulting from disqualifications, which Bradley estimates could be $140,600 per year. DPA also instituted initiatives to collect moneys owed it. Last fiscal year, more than $10 million was collected from providers as a result of audits of hospitals, nursing homes, pharmacies, laboratories and physicians. Between 1988 and 1992, collections rose from $43,230 million to $93,996 million from all sources. Most refunds came from providers who had overcharged the department for services to recipients. In effect, Edgar and Bradley today are biding their time because solutions to Illinois' problems are tied inextricably to the national health care situation. Illinois' medical welfare programs would be nonexistent without federal dollars. Once the Clinton health care and welfare proposals are known, expect Illinois to jockey for the most possible federal dollars. * Grace Kaminkowitz writes and consults about public affairs from Chicago.
March 1993 /Illinois Issues/23 |
|
|