|
Home | Search | Browse | About IPO | Staff | Links |
|
Home | Search | Browse | About IPO | Staff | Links |
|
Networking Consumer Health Information:
Elaine Russo Martin and Don Lanier Abstract The Library of the Health Sciences at the University of Illinois at Chicago obtained a grant from the Illinois State Library to implement a statewide demonstration project that would provide consumer health information (CHI) using InfoTrac's Health Reference Center CD-ROM database. The goals of the project were to cooperate with targeted public libraries and clinics in providing CHI at the earliest point of need; to provide access to the database via a dial-up network server and a toll-free telephone number; and to work with targeted sites on database training, core CHI reference sources, and referral procedures. This paper provides background information about the project; describes the major systems and technical issues encountered; and discusses the outcomes, impact, and envisioned enhancements. INTRODUCTION Health sciences librarians and health professionals have observed a proliferation of consumer health information (CHI) in the last decade. It is safe to say that, in many instances, librarians have been the primary proponents of new CHI databases or improved delivery capabilities. In other cases, the driving force behind the development of data has been the patient. The development of many new technological applications during the last decade made it possible for end users (consumers) to access CHI data without the services of an intermediary, whether librarian or health professional. End-user systems range from interactive work stations that support health education, patient decision making, and preventative practices to online self-help support networks and a variety of modem- and telephone-based systems. Preliminary studies suggest that these new programs can help cut health care costs and extend services while also improving the quality of care. One end-user system was implemented by the Library of the Health Sciences (LHS) at the University of Illinois at Chicago (UIC). The library received an LSCA Title III grant from the Illinois State Library to implement a statewide demonstration project that would provide consumer health information using Info-Trac's Health Reference Center (HRC) CD-ROM database. Project participants were located in Chicago, Gibson City, Peoria, Rockford, and Urbana. The goals of the project were to • cooperate with targeted public libraries and clinics in providing CHI at the earliest point of need;
• provide access to the HRC database via a dial-up network server and a toll-free telephone number;
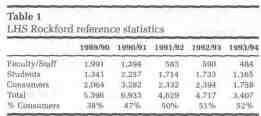
• work with targeted libraries on HRC database training, core CHI reference sources, and referral procedures. This paper focuses on system specifications and installation and on progress to date regarding network operations, use, and performance. The paper also discusses some of the long-term consequences of bringing the patient into the medical information loop. BACKGROUND The demand for consumer health information is increasing. Assigning responsibility for individual health care has shifted from the traditional approach of just a few years ago to a patient-centered one. In the 210 traditional approach, health providers typically offered services and information from an authoritative stance, with little patient interaction. Now, networking, both with and without the aid of computers, has been documented as an effective method of improving patient access to health information [1]. One study concluded that health consumers now actively participate in the medical decision-making process [2]. Another study of consumers in Canada found that 35% had used a public library as a source of health information [3]. A survey of Illinois residents focusing on library issues found that 8% (the highest percentage for any query category) of job- or business-related inquiries at public libraries concerned medical information [4]. Gibson and Kapp, in describing patient education considerations in rural practice, stated: "Essential to any effective patient education program is determining patients' needs and locating, evaluating, and utilizing appropriate resources" [5]. Masten and Conover reported on a project that involved automating both continuing education for health professionals and patient education, and concluded that health care providers and patients are benefitting from knowledge provided by computer-assisted and computer-managed instruction [6]. Humphries described a project aimed at providing CHI in collaboration with other institutions (public and community college libraries); the services included a networked version of the HRC CD-ROM [7]. One of the more comprehensive efforts to include the consumer in the health care process was the recent National Conference on Consumer Health Information [8]. Among the presentations were Telecommunications in Managed Self-Care, Interactive Health Systems, The CHESS Program, Healthwise Consumer Medical Knowledgebase, and American Self-Help Clearinghouse. In addition, health forums on commercial online services were described. The report of this conference included a series of consumer health informatics "vision statements" in which presenters and other experts summarized their "most pressing concerns" about the subject. A primary observation to emerge from the conference was that, within the next decade, consumer health informatics will play an important role in reinventing the nation's health care system. The University of Illinois at Chicago and its regional health sciences campuses in Peoria, Rockford, and Urbana offer an ideal environment in which to conduct a demonstration project aimed at providing CHI to underserved areas. Of Illinois' 102 counties, 84 are considered rural by the Center for Rural Health of the Illinois Department of Public Health [9]. For its program purposes, the center defines a rural county as one that is not a part of a metropolitan statistical area, as defined by the U.S. Bureau of the Census; or one that is a part of a metropolitan statistical area but has a population of fewer than 60,000. Between 1985 and 1992, the number of physicians of all specialties practicing in rural counties dropped by 4%, while the number practicing in urban areas increased by 16%. All or parts of thirty-five rural counties (41%) are designated by the U.S. Department of Health and Human Services as Health Professional Shortage Areas (HPSAs), indicating that there is only one primary care physician to serve 3,500 or more people. Ironically, Illinois graduated the third-largest number of physicians of any state from 1980 through 1992. During those years, Illinois had the third-largest number of citizens living in HPSAs of any state. In 1992, the underserved population of New York increased, moving that state into the third-highest ranking and bumping Illinois to fourth. Forty-eight rural Illinois counties lack a practicing obstetrician. Forty-one rural counties lack hospital obstetrical units, either because there is no hospital at all in the county (in twenty-two counties), or because the hospital has discontinued its obstetrical services. Illinois residents have a pressing need for health information. The state's infant mortality rate is 11.3 per 1,000 live births; only ten states have a higher rate. The Illinois death rate is 886.7 per 100,000 residents, higher than the United States average of 866 deaths per 100,000. Only five states have a higher number of residents with AIDS [10]. (All these data are as of 1992. Preliminary 1993 data suggest some improvement in the infant mortality rate.) While the cities of Peoria, Rockford, and Urbana are not underserved communities per se, each is located close to counties so designated. The authors envision that the CHI project reported in this paper will provide substantial assistance in expanding the use of appropriate resources by health information consumers in underserved areas. Data related to "consumer use" of the LHS in Rockford illustrates the key role the academic medical library plays in the provision of consumer health information to the community. Table 1 shows that approximately 50% of total reference use is related to consumer needs, up from 38% in 1989/90. The LHS in Peoria has experienced a similar pattern of consumer use, according to a study done by Landwirth in 1988 [11]. Annual report data for all UIC LHS sites suggests that the fifty-fifty split in affiliated versus unaffiliated reference use is valid university-wide. The Association of College and Research Libraries of the American Library Association recently published Library Services for Non-Affiliated Patrons, noting that " [a] review of the literature indicates that as many as 50% of all reference questions at large academic libraries come from non-affiliated patrons" [12]. 211 THE PROJECT The project was carried out in phases. The first step was to purchase and install equipment and arrange for telephone connections. A personal computer, modem, and printer were purchased for each site participating in the project—four medical libraries, three public libraries, the UIC Hospital, and Mile Square Clinic. Each site worked out the details concerning the location of its consumer health workstation. Also required, of course, was installation of a file server and networking that would make the databases available to participants. The file server network was located at the UIC LHS in Rockford because this library was involved with another CHI demonstration project and offered a much simpler network installation environment than existed at the UIC Chicago campus. Communication and training constituted the next major step in the project. To ensure that the program ran smoothly, a librarian from each LHS site was designated the liaison to the public libraries and other participants. Each designated librarian was responsible for communicating with participants and answering questions about the CHI workstation, training personnel at each site, following up and resolving all issues that arose, and providing brochures and documentation. Participant sites also designated a contact person responsible for communicating with the respective LHS liaison, reporting any problems encountered while operating the CHI workstation, scheduling training sessions, making sufficient copies of brochures and documentation, and providing supplies and evaluation forms for each CHI workstation. In addition to the LHS liaison and participant contacts, the principal investigator (PI) for the project assured communication with directors at participating sites to ensure that the project ran smoothly, participated in a series of planning meetings with liaisons and their partners, and reported quarterly and annually to the funding agency on project developments and progress.
The third phase of the project consisted in providing all project participants with access to CHI. Access included three principal components: computer database information, back-up reference service via the LHS liaisons, and document delivery. The primary thrust was to provide access to the computer database via the file server network. The key database was HRC, which provides three years of more than 150 consumer-oriented periodicals (100 with full-text coverage), more than 500 medical education pamphlets, and full text of five leading medical reference books. As the project develops, access to other databases may be provided.
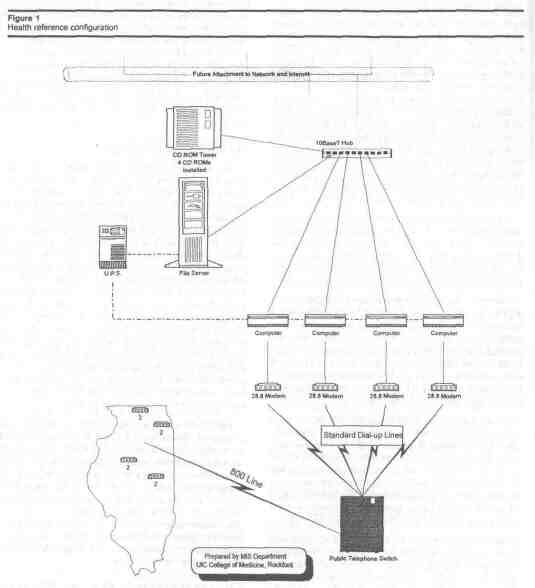
While the project centered on the provision of CHI using HRC on CD-ROM, other collateral services were included. During the period of the grant, document delivery and reference services were supplied by the academic health sciences libraries to the public library and clinic partners. Documentation for the project, entitled "Prescription: Collaboration for Health," was written by UIC librarians and supplied to each site and respective partner. This documentation provided essential information (procedures, forms, telephone and fax numbers, addresses) for effective document delivery, reference services, and referrals. Public library partners were also to be provided access to the UIC online public catalog and related borrowing services via the CHI network. Access to the Online Public Access Catalog (OPAC) was to have been provided with public access via the Internet. Since the project was initiated, university and Internet access policy has limited the passthru to university-affiliated persons with user identification and passwords. However, the provision of access to the OPAC for CHI partners remains an objective. The fourth and final phase of the project related to strengthening the partnership between the university and the community. This theme meshed well with LSCA goals and also with a major UIC initiative, the Great Cities Program. The project presented a model for partnership in an area vital to society: consumer health information. SYSTEMS AND TECHNICAL ISSUES The client-server network was developed by outside experts in this field. A client-server network is any application in which the requester of actions or information is on one system and the supplier is on another [13]. The system was designed with the help of the Management Information Services staff of the UIC College of Medicine at Rockford. In addition, reports about other server networks were examined and contact was established by phone or electronic mail with systems staff and project leaders at other universities. The systems and sales staff of Information Access Corporation was also consulted. Finally, once a fairly detailed concept was developed, Interserve Computer 212 Group, in Rockford, was consulted and subsequently submitted a proposal that was accepted. The primary hardware component of the CHI network server is a 486-DX2 66 file server with a 1.7 gigabyte hard drive, 32 megabytes of random access memory, a Video Graphics Array monitor, an Ethernet card, and Fast-SCSI controller. The file server also has a CD-ROM subsystem with a seven-drive bay tower installed with an EISA controller. The file server manages the requests for and delivery of data contained on the HRC CD-ROM. Another network component consists of four 386SX computers operating at 33 megahertz attached to four 28.8-baud Hayes-compatible modems for each dial-up line. This configuration supports some of the networking software and allows for higher processing speed compared to the original design utilizing only one computer as a remote access server. The system also provides a layer of network security, protecting against both intentional intrusion and electrical disturbance. Other hardware components of the file server system include a D-Link 16-port 10BaseT concentrator, a transceiver and cable connecting the backbone to the Thinnet, and a 900-volt uninterruptable power supply. The file server, the four computers with modems, and the CD tower are all connected to the 10BaseT hub. Software acquired for the server includes Novell 4.01 for up to twenty-five users, LAN WorkGroup 4.2 for up to twenty-five users, ICE/TCP software for workstations (to access Novell and Unix), and a ten-user network license for PcAnywhere communications software. At the time of acquisition it was not known if all the software would work with the system, but the hope was that if one package did not work as planned, then an alternative could be used. Telecommunication links for the file server consisted of an "800" dial-up number for four lines connected to the server. A primary objective was to make network access as easy as possible through the use of simplified commands and fast, reliable performance. For the demonstration project, dial-up service was more feasible than full Internet access because only eight sites were involved and Internet connections were not considered an option at some sites (see Figure 1). To access the server, each project participant was given a computer, monitor, modem, and ink-jet printer. Participants were responsible for the installation of their own phone lines. Each participant was also given a copy of PcAnywhere, including telephone numbers and connection and installation instructions. This software permits remote access to and control of the host server. There were several delays in the process of setting up the CHI client-server network. Problems encountered included the delayed release of grant funds, difficulties in arranging for systematic communication among the project partners, the lengthy requisition and purchase-order turnaround time, a holiday break, and miscommunication between the installer and the computer maker about pricing. As noted earlier, the original configuration called for only one computer as a remote-access server, but it performed at an unacceptable rate of speed; thus the transition to four servers. The CHI network was installed and the first dial-up connection was made on April 6, 1995—about six months after funds were made available and accounts established. PLANNED ENHANCEMENTS The vision for the CHI project did not end with grant funding. A second LSCA grant proposal was submitted with the aim of expanding the number of partners and providing Internet access. It is hoped that the second phase will provide information directly to the consumer and establish a statewide network providing reference and full-text document delivery services to Illinois citizens. Specific objectives of the second grant proposal, which has been approved, are to identify and document existing and new cooperative arrangements for providing CHI among the health sciences libraries, public libraries, and health care facilities in the state of Illinois; to train public librarians and hospital and clinic representatives in the use of CHI resources and the Internet; to expand the number of sites to include Southern Illinois University, a Chicago public library, and a hospital with a patient-education focus; and to provide citations, full-text documents, referrals, directories, and other types of health-related reference services directly to the citizens of Illinois. Librarians and health professionals recognize the great need of consumers for health information that is up-to-date, understandable, and easily accessed. We hope that the CHI project will be only the first step in the provision of health information. Envisioned subsequent steps include, but are not limited to, the provision of Internet access to allow more users and easier connection for some sites; acquisition of a site license allowing increased numbers of simultaneous users; access to other databases; and coordination of CHI access and rural medicine initiatives now taking place in certain regions of Illinois. THE CONSEQUENCES OF BRINGING THE PATIENT INTO THE INFORMATION LOOP There are consequences of bringing the consumer into the health information loop. However, the trend is well established, having originated at least a generation ago and culminated in the Patient Self Determination 213
214 Act of 1990. A 1961 study found that 90% of physicians did not inform patients of a cancer diagnosis while another in 1979 found that 97% of physicians preferred to inform patients of this diagnosis [14]. Such a reversal in the attitudes of physicians is dramatic.The information age and progress in civil rights have many roots in common, and there can be no turning back on the road to patient empowerment. One of the most difficult barriers to overcome in bringing the patient into the information loop is the amount of time health professionals must devote to providing full information regarding diagnosis, treatment options, and likely or possible side effects. It may be argued that such disclosure will increase costs substantially but influence outcomes only minimally. The present authors hope that the CHI project and other initiatives across the country will contribute to the patient information resource base and reduce the chances that health professionals will increase their fees. In fact, it may be that the amount of information available is not the issue. Rather, what may be most needed, is the interpretation of information available. By and large, available medical information is technical and full of jargon. The consumer cannot be expected to understand it. The content of HRC, on the other hand, is aimed at the consumer. Likewise, the consumer may find the literature of nursing and other allied health disciplines more helpful than that of clinical medicine. In the authors' view, the consequences of bringing the patient into the information loop can be described as follows: In sum, providing relevant information directly to the consumer is a low-cost way to enroll the cooperation of the patient in the decision-making process. The information can be read and digested after the medical visit. Information can facilitate patients' regaining a sense of control about their health and their choices, and reduce some of the stress that occurs when dealing with serious medical problems [15]. CONCLUSION There has not yet been sufficient use of the UIC system to evaluate fully its performance and user response. However, preliminary observations are that dial-up access is quick and easy and the performance of the networked version of HRC is equivalent to that observed with a stand-alone workstation. Evaluation forms have been made available at consumer health workstations at each site. From April through June 1995 a total of 131 evaluations were completed. Of those responding from any LHS site, 93% found the workstation easy to use, while 29% would have liked more instruction. A total of 88% said the information they received answered their question, and 31% said the information would change their behavior. Almost the same percentage, 34%, said the information they received gave them a question to ask their physicians. Of those responding at any LHS site, 51% were students, 4% were health professionals, 9% were patients, 10% were relatives or friends of patients, 2% were caregivers, 4% were business people, and 11% were library staff. Of the thirty-nine respondents from the public libraries, 89% found the workstation easy to use, and 5% would have liked more instruction. The system answered the questions of 61% of users, 18% said the information would change their behavior, and 18% said the information gave them questions to ask their physicians. Of those answering from the public library, 41% were students, 2% were health professionals, 5% were patients, 2% were relatives or friends of patients, 15% were business people, and 31% were library staff. For both LHS and public library patrons, the average time spent per session ranged from ten minutes to thirty minutes. Comments were very positive. Representative comments were: "very good information," "very helpful," "wonderful asset for any library," "very user-friendly," "program is terrific," "most useful source found yet," and "staff very helpful." There were very few negative comments. Two users said the screen quality could have been better, one person wanted the system to include photographs, and some were unable to log on when they wanted to. Both positive and negative comments will be helpful in making adjustments to existing services and planning enhancements. REFERENCES 1. RICHETELLE AL. Healthnet: Connecticut Consumer Health Information Network. Conn Med 1990;(11):632-4. 2. REES AM. Communication in the physician-patient relationship. Bull Med Libr Assoc 1993 Ian;81(1):1-10. 3. MARSHALL JG. A development and evaluation model for a consumer health information service. Can J Inf Sci 1992;17(4):1-17. 4. Illinois state library poll on library issues. Champaign-Urbana: Library Research Center, University of Illinois at Urbana-Champaign, 1961-1991. 5. GIBSON PA, KAPP CJ. Patient education in the rural practice. In: Yawn BP. Exploring rural medicine. Thousand Oaks, CA: Sage, 1994:240-52. 6. MASTEN Y, CONOVER KP. Automated continuing education and patient education. Comp Nurs 1990;8(4):144-9. 7. HUMPHRIES AW. Providing consumer health information through institutional collaboration. Bull Med Libr Assoc 1994;82(1):52-6. 8. FERGUSON T. Consumer health informatics: bringing the patient into the loop: First National Conference on Consumer Health Informatics, July 16-18,1993, Stevens Point, Wisconsin. Austin, TX: Self-Care Productions, 1993. 9. Rural health perspectives, [s.l.]: Center for Rural Health, Illinois Department of Public Health, 1994 Jan:3. 215 10. U.S. BUREAU OF THE CENSUS. Statistical abstract of the United States. 112th ed. Washington, DC; U.S. GPO, 1992. 11. LANDWIRTH TK, ET AL. Reference activity and the external user: confluence of community needs at a medical school branch library. Bull Med Libr Assoc 1988;76(3):205- 12. [News column]. Coil Res Libr News 1995;56(3):140. 13. MINOLI D. Analyzing outsourcing: reengineering information and communication systems. NY: McGraw-Hill, 1995:32. 14. DEBER RB. Physicians in health care management: 7. The patient-physician partnership: changing roles and the desire for information. Can Med Assoc J. 1994;151(2):171-6. 15. MARCUS SH, TUCHFELD BS. Sharing information, sharing responsibility: helping health care consumers make informed decisions. In:Safran C, ed. seventeenth annual Symposium on Computer Applications in Medical Care: patient-centered computing. New York:McGraw-Hill, 1993:3-7. Received June 1995, accepted August 1995.
APPENDIX A Hardware: 1. Compaq Prosignia File Server 1.7 gigabyte hard drive Intel 486-DX2 66 processor 32 megabytes random-access memory Video Graphics Array monochrome monitor built-in Ethernet and Fast-SCSI controller 2. Meridian Data CD-ROM subsystem seven-drive bay tower installed EISA controller up to ten concurrent users 3. Four 386SX book-size computers at 33 megahertz each with 28.8 external modem each connected to the lOBaseT hub 4. Hayes compatible 28.8 external modems for host computers and remote computers 5. D-Link 16-port 10BaseT concentrator 6. American Power 900 VA U.P.S. Software: 1. Novell 4.01 twenty-five user
2. PcAnywhere communications software, ten-user license 3. Lan WorkGroup 4.2 twenty-five user 4. ICE/TCP software for workstations to access Novell and Unix APPENDIX B Example of handouts prepared for partners University of Illinois at Chicago Library of the Health Sciences Prescription: Collaboration for Health Consumer Health Information Reference Sources The following list of sources was compiled from favorite reference sources of both public and health sciences librarians. With a medical dictionary and a selection from the following sources, it should be possible to provide information on a wide variety of consumer health requests. General Reference: American Medical Association Encyclopedia of Medicine. Charles B. dayman, M.D., editor. Random House, 1989. (0-394-56528-2). $45.
Current Medical Diagnosis & Treatment, 34th ed. Appleton & Lange,
Magalini, Sergio I. Dictionary of Medical Syndromes, 3rd ed. Lippincott, 1990. (0-397-50882-4). $99.
Mayo Family Health Book. David E. Larson M.D., editor. Morrow,
Merck Manual of Diagnosis & Therapy, 16th ed. Merck, 1992.
Professional Guide to Diseases, 5th ed. Springhouse, 1995. (0-874- 34769-6). $33. Physicians' Guide to Rare Diseases. Jess G. Thoene, M.D., editor. Dowden, 1992. (0-9628716-0-5). $72.50. (note: 2nd ed. due out 6/95) Drug Information—either: The Essential Guide to Prescription Drugs. James W. Long, M.D., and James ). Rybacki, Pharm.D. Harper Perennial, 1994. (0-06-271574-7). $35. (0-06-273211-0). pbk. $17. PDR Family Guide to Prescription Drugs, 2nd ed. Medical Economics Data, 1994. (1-56363-020-6). $25 pbk. The Complete Drug Reference, 1995 ed. United States Pharmacopeia, Consumer Reports Books, 1994. (0-89043-769-6). $40 pbk. (annual). Consumer Health Books, Associations, Hotlines: Consumer Health Information Source Book, 4th ed. Alan M. Rees, ed. The Oryx Press, 1994. (0-89774-796-8). $45. * Elaine Russo Martin, Assistant University Librarian for the Health Sciences, and Assistant Professor, Library of the Health Sciences, The University of Illinois at Chicago; and Don Lanier, Health Sciences Librarian at Rockford and Associate Professor, Library of the Health Sciences, The University of Illinois at Chicago. Reprinted with permission of the Medical Library Association from the April 1996 issue of Bulletin of the Medical Library Association. This paper is a revision of a presentation to the CIC Rural Datafication Third Annual Conference, Indianapolis, Indiana May 23, 1995, and to the Ninety-Fifth Annual Meeting of the Medical Library Association, Washington, D.C., May 10, 1995. Funding for the project was provided by the Illinois State Library, a division of the Office of the Secretary of State, using federal Library Services and Construction Act funding. 216 |Home|
|Search|
|Back to Periodicals Available|
|Table of Contents|
|Back to Illinois Libraires 1996|
|