|
Home | Search | Browse | About IPO | Staff | Links |
|
Home | Search | Browse | About IPO | Staff | Links |
|
By JENNIFER HALPERIN
Chicagoland business leaders
With health costs on a ballistic path, this group
Imagine a health care future that includes not only insurance for everyone who needs it, but information at one's fingertips regarding the quality and cost of a whole host of health care providers and their procedures. Both of these are tall orders to fill and the first obviously depends on President Clinton's ability to steer his health care proposals to success. But a group of executives at large employers in the Chicagoland region has begun trying to tackle the second notion one that would put together information for employers of all sizes on the types of medical services received by their workers. The charges and outcomes of these services would be tracked as well, providing health care customers the ability to make what could be better-informed decisions on how and where they get medical care.
Long before President Clinton took office and convened his health care task force, Paulus and other business executives began mulling health care problems and potential solutions on a regional level. "I had talked to a [Washington official] who said several business leaders had come to him wanting government to do more to control health care costs," Paulus said. "My concern was that as a matter of good public policy, it may not cost less if government was running things." After the group's initial breakfast meeting nearly three years ago in Chicago, members decided they needed a "snapshot" of the region's health care status. The state and Chicagoland chambers of commerce had become involved, along with a few dozen major employers such as Ameritech. Money was raised to fund a $20,000 study by the University of Chicago's Center for Health Administration Studies. The study's results, Paulus said, confirmed what many of the executives already had feared: Health care costs in the Chicago area will grow exponentially over the next several years. "It showed that the system can't be supported indefinitely," he said. "It was not a surprise, but it's nice to see it documented." Among the report's elements that caught the business world's eyes:
In just eight years the average cost per employee of providing health care benefits more than doubled. "Health care costs are growing extremely fast in the mid- to high teen percentages a year," said Henry S. Webber, one of the study's authors. "At that rate, it doesn't take too many years to see huge increases. In 1980, which wasn't exactly the Dark Ages, employers' costs were about $700 or $800 per employee. In 1991 they were up to $3,600, and I'd say now they're over $4,000."
16/October 1993/Illinois Issues
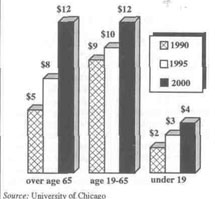
covered by Medicare or Medicaid onto those insured privately. For example, if a hospital provides $1,000 worth of treatment to a Medicaid patient but is reimbursed by Medicaid for only $900 of that treatment, it likely will shift the remaining $100 cost to privately insured patients, such as those insured through their employers. The study's authors estimated that cost-shifting in the Chicago area cost private employers $1.9 billion in 1990 a figure they said could climb to nearly $7 billion in the year 2000 if no health care reforms are implemented. In general, the report found that Chicago and Illinois are close to the nation's average on most measures of health care cost and access. "The study found Chicago is basically average on some indicators," Mortimer said. "Are we satisfied with that? Do we want Chicago to be average? Or do we want to be superior?" The study's authors had a few recommendations that while perhaps not guaranteeing Chicago a superior health system perhaps could help ward off the monstrous health care cost increases employers face. "These are not recommendations that would solve all problems; they're not a cure-all," Webber said. If all six were adopted, he said, they could reduce the rate of growth of medical costs but would not lead to a reduction in cost from current levels. They would shrink but not eliminate the problem of uninsured people through efforts such as encouraging small businesses that otherwise may not be able to afford health care for employees to participate in a health care network with the larger ones. But for starters, the coalition decided to undertake just two of the recommendations, putting off decisions on the others until details of Clinton's health care package have been made clear. One recommendation the coalition has begun working on would lead to the scenario mentioned above, in which information on quality and costs of various health care procedures would be available. It involves development of a database on medical services received, outcome of these services and the amount charged for the services. Employers could pool data they already have from employees' health care claims, Webber suggested, or they could mount an effort to expand upon the hospital data already compiled and published by the Illinois Health Care Cost Containment Council to include information on other medical services.
October 1993/Illinois Issues/7 same rates. "Most health plans are now 'experience rated,' under which those with old, sick people are charged more money," Webber said. "We believe community rating moves back to what insurance should be spreading risk rather than searching out groups with the best risk. But not every coalition member agrees with this." Another recommendation calls for businesses to support insurance reform through community rating and legislation that would eliminate or modify the Employee Retirement and Income Security Act, or ERISA, presumption. ERISA has exempted large, multistate employers from state health care laws. According to the study, "The only community in the United States where over 90 percent of the insurance market is community rated Rochester, N.Y. also has health costs which are one-third under the national average." The final recommendation urges Chicago's business community to support legislative efforts to offer no or low-cost health insurance for all children under 18 in Illinois. This proposal would be "an important part of the solution to the problem of inadequate access to primary care for part of the population," the study's authors wrote. "It seemed like safety was the issue for companies to pay attention to in the '80s," said Joe Leutzinger, manager of health promotions for Union Pacific Railroad. "Now, in the '90s, health is the main issue." And with good reason. Just as consumers have been hit in their wallets by rising health care prices, employers have had their pockets hit as well: While health benefits took up 26 percent of private sector employers' net earnings in the United States during 1984, they ate up 45 percent of those earnings in 1990, according to the Center for Health Administration Studies at the University of Chicago. "Those are ratios that have impressed some of the people in the boardrooms," said Jim Mortimer, president of the Midwest Business Group on Health, a coalition that aims to help employers improve the quality of health care. "They used to view health plans as a minor expense almost something to be given away as a freebie in bargaining with labor unions. Now it's a significant cost of doing business." And, as Paulus said, the Chicago regional coalition would like to keep those "significant costs" from rising by making individuals better consumers of health care. If the president's proposals leave enough latitiude for local initiatives, he said, "you'll see this Chicago coalition take off at a fast pace." But Paulus does harbor some concerns about details of Clinton's plan. "It may not have the focus of individuals' responsibility to seek out the best, most cost-effective care," he said. "In the Clinton administration's attempts to reduce costs . . . I'm concerned that entrepreneurs in the medical field won't be encouraged by what that system contains. For example, I do sense that if the Medicare concept is translated to cover everyone, you'll get a good doctor who feels the whole thing is too bureaucratic and may take early retirement." Ray Werntz, vice president of compensation and benefits for the Whitman Corp. holding company and a member of the business coalition, agreed. He said employers would be wise to place a high priority on instilling employees with "values and skills people need to develop to become 'model' patients." "It covers a wider range of skills besides not smoking," he said. "You've got to help doctors and patients work together as efficiently as possible. To do that, you need patients of a certain type first of all, people who really have a health problem, people who can articulate their problems, people who can follow treatment programs and people who can avoid health problems." This is more valuable in the long run, Werntz said, than merely putting managed health care networks in place in an effort to save money. "There's a difference between managing care and managing people," he said. "By managing care you may get good care, but you're not necessarily giving skills to patients. I still think a day will come that we can get rid of this micromanagement of health care, although that may not be within my lifetime. Our dream is to eliminate reasons health care has to be managed." This concept represents a huge shift in thinking on employers' parts, he acknowledged. "To get costs under control, the business world has been trying to control what a person's going to get. They've been trying to force health care providers to give them a deal. But using economic leverage to get discounts may be a short-term gain. I think the employer strategy of relying exclusively on controlling care is effective for a while, but in the long-term it can be harmful to the medical system. "We have a problem in this country with the long-term," he said. "We're deeply concerned about what it costs today. Whether we're talking about education, health care or anything else, we've got that short-term/long-term conflict, and this just highlights it." Paulus pointed out that employers may not be the only ones who will have to undergo a shift in thinking about health care. "We may have to change Americans' expectations of receiving only excellent care," he said. "That doesn't translate into them receiving poor or below average care, but maybe 'good care.' " Werntz said he is encouraged by coalitions like the one in Chicago, where employers "are trying to deal with health care on a higher plane not just trying to negotiate discounts but trying to develop rational ways of measuring managed care networks, like through the database they're working on." But even beyond databases and fitness programs and everything else employers can do to educate their employees on how to be wise medical customers, Werntz said the success of health care reform likely will depend on even larger issues for society as a whole. "Generally speaking, people are most concerned about health care if they have other things in their lives pretty much in place," Werntz said. "If you don't have a decent place to live or enough to eat, you're not going to have healthy habits as a top priority." *
18/October 1993/Illinois Issues |
|
|