|
Home | Search | Browse | About IPO | Staff | Links |
|
Home | Search | Browse | About IPO | Staff | Links |
|
By ANTHONY MAN
Pharmaceutical Assistance Program:
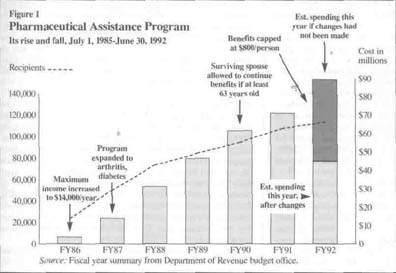
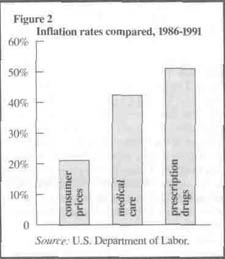
It was midnight at the University of Chicago campus, almost two hours into a live ABC television "town meeting" on health care, when audience member Rae Williams stood at a microphone. "I'm a diabetic, I have a heart problem, I'm a cancer patient," she told the national TV audience. "But my biggest problem," the 82-year-old continued, is the cost of medicine. "What does one do when they're living on a fixed income of $6,000 a year? How can I pay $218 a month for medication?" From mid-1985 until last summer, the state of Illinois had the answer. The state provided help for elderly and disabled people who had low or moderate incomes and needed to buy certain kinds of medicine especially expensive cardiovascular medication. The Pharmaceutical Assistance Program was popular with beneficiaries, who paid a pittance for an unlimited quantity of medication, and with legislators, many of whom passed out applications from their district offices to curry favor with the recipient-voters. For a time, everything was fine. The program cost just $3.8 million in its first year, fiscal 1986. But by early 1991 when Gov. Jim Edgar arrived in office, continuing the plan as it was would have cost a whopping $90 million in fiscal 1992. For the new administration and some legislators, the state of the pharmaceutical program was the epitome of government failure: a worthy idea begins small and then balloons. Political science textbook theory aside, it also presented immediate budgetary and political problems for the new governor grappling with a fiscal crisis. "We've taken on programs that are very nice, but we don't have the ability to keep them up," said Edgar's budget director, Joan Walters. "To me, it's irresponsible to set up things which inevitably you're not going to be able to sustain. This is an example." Douglas L. Whitley watched formation of this and other programs as president of the Taxpayers' Federation of Illinois. He now administers pharmaceutical assistance as director of the Department of Revenue. "It's a classic example of what would be nice to do and gracious to do and there is a need," Whitley said. "It was an attractive program. I don't think that people necessarily recognized it as a social program with a potential for growth that it has had." Even someone who enthusiastically supports providing state help to buy medication, Sen. Penny L. Severns (D-51, Decatur), said that the program "has grown bigger and faster than anyone imagined when it was enacted a few years ago." From fiscal 1986 to 1991 the cost per prescription went up 44 percent and the number of recipients increased 392 percent. Overall spending soared 1,743 percent. (See figure 1.) Dawn Clark Netsch, now state comptroller, helped create the program when she was a state senator. She said the growth demonstrates there was a need. "We no longer have a societal, charitable, familial structure that takes care of all those things," she said. "We have things that keep people alive who would have not been able to stay alive a few years ago. Who's going to help them if we collectively don't? Government is us. It's not some horrible big ogre standing up there beating us into submission. It's us, and one of the reasons it does so much is because it is sort of our collective conscience." Conscience is expensive. In the frugal environment of the 1991 legislative session, the General Assembly ultimately went along with Edgar's proposal to cut the pharmaceutical assistance budget almost in half. The changes capped the state's exposure but did little to reduce the cost of an individual's medication, and people like Williams are feeling the effects. "I've reached the cap in five and a half months," Williams told the television audience. "Therefore I have to pay strictly cash for all my medications now, and that comes to $218 a month." Williams is not alone. When she spoke the night of February 6, more than 4,400 people had "capped out" a bit of jargon used by the people who run and watch the program. The most recent estimate from the Department of Revenue predicts from 20,000 to 25,000 people will hit the cap by June 30, the end of the fiscal year. One positive development: Fewer people began hitting the caps as early as estimated, possibly because of new cost-saving incentives, possibly from a greater awareness among beneficiaries of the need to control costs. Discussion of the effects of reducing pharmaceutical aid is a sharp departure from the debates since the early 1980s. Back then, Netsch and then-Rep. Woody Bowman, now fiscal adviser to Cook County Board President Richard Phelan, attempted to establish a broad-based system modeled after a New Jersey effort that covered all prescription medication. Failing at that, the sponsors got a smaller plan, covering only cardiovascular medication. The American Heart Association calls high blood pressure "the silent killer." Uncontrolled, it often leads to stroke or heart attack, but medication must be taken frequently and is expensive. 18/April 1992/Illinois Issues Then-Gov. James R. Thompson bought the scaled-down version. For an $80 annual fee, elderly or disabled people with yearly household incomes of less than $12,000 could get a pharmaceutical card. A person could present the card at a pharmacy and get a month's supply of whatever cardiovascular medicine was prescribed. The state paid. "Pharmacists told us we were the Cadillac," recalled Darlene Logsdon, program administrator at the Department of Revenue. In the first six months, the state spent $796,000 on prescriptions. Including administrative costs and pharmacist fees, it worked out to $94.69 for each of the 8,406 participants from July through December 1985. Full fiscal year expenses were $3.8 million. Rep. Joel D. Brunsvold (D-71, Milan) issued a press release in March 1986 touting the results, described in the release as "well under the Thompson administration's projected cost estimate of $5 million per year." That May, Netsch told colleagues the plan was in great shape financially. She said at the time, "We were given all sorts of wild estimates of what it would cost the state, that it would bankrupt the state. I just don't think the costs are going to run amok." She was wrong, though not alone. Participation and costs soon soared, sometimes caused by forces beyond the state's reach, sometimes by factors the state could control but did not. First, in 1986, participants' maximum household income was raised to $14,000, enlarging the size of the applicant pool. Also, word began spreading about the benefits, and the population was aging. Enrollment began a sharp and steady increase. In subsequent years, legislators engaged in an annual spring ritual of introducing bills to expand the kinds of drugs the state would pay for. Some proposals were limited to coverage of specific ailments such as Parkinson's disease, epilepsy, glaucoma or even the need for hearing aids. Others would have covered all or almost all prescriptions. Still others sought to expand eligibility to people with higher incomes. Most went nowhere, although coverage was expanded to diabetes and arthritis. Critics frequently mention expansions, contending the practice of starting a limited program and later expanding it is one of government's big problems. Even though arthritis medication makes up only about 12 percent of spending on the 30 most dispensed drugs, those who are most disturbed by the escalation of the program frequently cite arthritis medication. They argue that arthritis is not life-threatening, in contrast to the other covered diseases, although they concede arthritis can affect a person's quality of life. Despite the criticism, expansions of the program were not as frequent and far-reaching as some seem to believe. One clear problem was inflation in prescription drug prices. U.S. Department of Labor figures show that inflation in the cost of prescription drugs outpaced even the extraordinarily high rate of medical inflation from 1986 through 1991. (See figure 2.)
All factors conspired to make the program a budgeter's nightmare. By fiscal 1991, the state spent $70.2 million on 108,426 recipients. When Edgar took office in the midst of a budget squeeze with a promise not to increase taxes, his staff was presented with the $90 million estimate for fiscal 1992. "We went in asking for an amount that didn't exist," Logsdon said. "That's when the governor's office said, 'Do something.' We were in serious trouble." Walters said the growth in this and other health-related social efforts is so great that unless controlled they could "completely take over the rest of state government." Edgar called for a strict limit on the amount of help each participant could get. He suggested a $400-a-year cap on benefits about two months for Rae Williams. As one relatively small piece of a budget proposing significant social service cuts, the pharmaceutical reductions attracted relatively little attention. By all accounts, the strongest lobbying effort was waged by pharmacists. "Even at the end of the legislative session, when the bill was being passed, the people who were in there were not the senior citizens; it was the pharmacists," Whitley said. Eventually, per person expenditures were capped at $800 for the fiscal year, rather than $400. Also, a copayment of $5 was required for each generic prescription and $10 for each brand-name prescription. Aside from the cap, which is purely cost containment for the state, the changes include a significant reform, which also happens to save money. Despite objections from manu- April 1992/lllimis Issues/19 facturers of brand-name pharmaceuticals, there are now greater incentives to use generic drugs. The copayment is doubled for brand-name drugs, and participants must pay the difference in price between the generic and brand-name if a generic is not used. The state also greatly expanded the number of generic drugs recognized as acceptable to the program. Before the changes, there was little incentive for beneficiaries to consider the number of prescriptions or the cost of the drugs. Requiring people to pay something "tends to bring about a more appropriate use," Walters said. She said the change might encourage people to question doctors more closely about their recommendations. "Elderly people in my experience tend to be very frugal, very careful about their expenditures. They come from an era when you didn't use things unwisely, and it may cause some of those responsible questions to be asked of medical providers, probably good questions," Walters said. Organizations representing participants said little good, and much harm, is the result. They contend the social cost, and ultimately the economic cost, of the cut will be staggering. Rep. Janice D. Schakowsky, (D-4, Evanston), former executive director of the Illinois State Council of Senior Citizens, said it is a mistake to look at the pharmaceutical program's costs in a vacuum. She said it "has been a lifesaver for many seniors and a benefit for the state" by reducing the number of strokes, amputations from diabetes and disabling effects of arthritis. Schakowsky and others believe capping benefits means people will have to choose whether to buy food or medicine. They also argue the savings will be dwarfed by the eventual cost of caring for people who will require hospital or nursing home care because they did not have enough medicine. "We are postponing, and not for very long, high medical bills that the state and federal government are going to have to pick up," said Madeleine Solomon, director of public policy for the American Heart Association of Metropolitan Chicago. Solomon labeled the cut foolhardy. That argument does not persuade Walters, who said she has never encountered a social service advocate who does not claim any kind of cut will somehow drive up long-term costs. "That is a given statement that everybody will make no matter what we do," she said. Even Jason Kay, Schakowsky's successor as executive director of the senior citizens council, said such reasoning is used so often it has lost its appeal: "Legislators and policymakers have become hardened to it." Yet several activists pointed to an article published last October in the New England Journal of Medicine describing what happened when New Hampshire capped the number of prescriptions its Medicaid plan would buy. Nursing home admissions doubled, Harvard Medical School researchers found, then fell when the prescription limit was lifted. The administration countered that people who are losing pharmaceutical assistance are not without alternatives. Eventually, if a person is poor enough, help is available from the federal-state Medicaid program for the poor. Michael Belletire, one of Edgar's executive assistants, conceded that becoming poor enough for Medicaid can mean significant lifestyle changes for people, especially the elderly who may have to move. Some pharmaceutical manufacturers are willing, on a case-by-case basis, to provide free or low-cost medication for patients who cannot afford it, advocacy groups, legislators and doctors said.
Nevertheless, opponents of the state cuts argue that deaths will be the ultimate result. "There is absolutely no question that people will die," Schakowsky said. Kim Bauer, planning supervisor for the Suburban Area Agency on Aging in Cook County, said people are asking the questions, "Should I eat or take my medicine?" or "I have $500 coming in a month and my medicine costs $300; do I stop taking my heart medication or my diabetic medication? Which will I die from first?" Such rhetoric is not far-fetched, according to Sen. Frank Watson (R-55, Greenville), a pharmacist. He said, "There are some people who are discontinuing medication. I'm aware of several cases where people are taking medication instead of two or three times a day taking it once a day." While not dismissing the importance of individual lives, Whitley strongly rejects setting government policy because of specific, individual cases. "Government should not be run by anecdotes. Government should be run by the averages and the mediums. There are always going to be outliers. There are always going to be problems, there are always going to be fundamental breakdowns, and it's not a perfect situation." Walters said government cannot be an all-protective parent. "People can die from a multitude of things, every single day. Part of living is dying," she said. "There are people dying this very minute because they are poor, because they got run over by a drunk driver. There is not enough money in the world to ensure that people will not have risks and face them every day." The Edgar administration is considering refocusing the program to help people with the greatest need. Rather than providing each recipient with a set amount of assistance, $800 this year, the program might be turned around to provide catastrophic coverage. After paying for some drugs themselves, people who have high prescription bills would have all or part of the rest paid by the state. Under one scenario, a person would have to pay for the first $200 of prescriptions. Beneficiaries and the state would split the cost of additional medication until $800 in charges is reached. The state would then pick up all costs over $800. Such a change would arguably cover those who need help the most because they have the greatest need for expensive medication. Such a change might be politically difficult, however, because many people who got something in the past would get nothing. Yet Whitley thinks it would be the best way to target a limited 20/April 1992/Illinois Issues amount of money. "I don't think that we have to take everybody from day one and carry them through. I think it's more important that we are able to pick up the person who is most likely to be in jeopardy," he said. "I just don't happen to accept the peanut butter approach to politics, which is that you give everybody a little bit. You spread it so thin that there's something for everybody, but you don't do anything well. You need to determine what your programs are, what your priorities are, and put your money there." Politics aside, the Heart Association's Solomon said such a move is unworkable because many participants could not afford the first few hundred dollars that would enable them to get state assistance. "It's a barrier for people. They can't pay that much," she said. While that is undoubtedly true for many recipients, it is not necessarily true for all. Besides age and disability, the only qualifying factor is a household income of $14,000 or less. A single person with an annual income just below $14,000 is in a much different position than a couple with a household income of $10,000. One suggestion from some members of a special House-Senate committee studying the program is to provide benefits on a sliding scale, with the greatest aid going to those with the lowest incomes. Another variation would base benefits partly on applicants' assets, which are not currently a factor in eligibility.
Targeting the assistance to those with the greatest need may not be the best move politically. Some suggest pharmaceutical assistance would never have been cut if it had a broader base and reached significantly into the middle class. That might have made it politically untouchable, like Social Security at the federal level. Netsch said the pharmaceutical cuts did not generate a political outcry because they affected "limited-income people and they are not always as well-organized or have as loud a voice, unfortunately. But many of them need help much more than people who get Social Security." Even the most ardent advocates for the pharmaceutical plan do not expect higher taxes to provide a solution, although some tax and pseudo tax measures are under consideration by the special House-Senate committee studying the program. Among the ideas that have been floated: Removing the sales tax exemption for certain drug items such as toothbrushes or anti-dandruff shampoo. That might raise $45 million a year.
Requiring pharmaceutical manufacturers to rebate to the state a percentage of their sales of drugs bought by the program. Connecticut expects to raise $2.6 million this way, and New Jersey is considering it, with an estimated benefit of $16.6 million. In both cases, manufacturers' rebates are estimated at 10 percent of the programs' spending on drugs. Cutting the companion Circuit Breaker tax relief program. Eliminating the $80-per-household grant would save about $20 million a year. (The tie to tax relief is the link to the Department of Revenue. Whitley has recommended transferring pharmaceutical assistance to a human service department such as public aid or aging.) Increasing the amount of medication a beneficiary can receive at one time. If people could fill prescriptions quarterly instead of monthly, they would save money on copayments. Pharmacists would lose under such a change because they get a $3.60 dispensing fee each time a prescription is filled. The fee comes out of each participant's $800, so with less frequent refills, they could get more medicine. The legislative committee expects to meet its early April deadline to recommend proposals (for committee members, see box). At the same time Edgar is scheduled to unveil his proposed budget for fiscal 1993. Early April is also the time when more and more beneficiaries will be reaching their caps in pharmaceutical assistance. Their advocates promise to use the recipients' pain to influence the legislature and the governor in the shape of the program for fiscal 1993. Those who favored and opposed last year's action expect lots of attention on the topic this spring. As Walters put it, "This is the kind of issue that, face it, it's an election year. Everybody in the General Assembly is up. Everybody's got old people in their districts, and I think there's probably a lot of interest in showing the demonstration of concern to this population." Anthony Man is the Statehouse bureau chief for the four Lee Enterprises Inc. newspapers with readers in Illinois. He writes frequently about health care policy. April 1992/lllinois Issues/21 |
|
|