|
Home | Search | Browse | About IPO | Staff | Links |
|
Home | Search | Browse | About IPO | Staff | Links |
|
Is there a doctor in the house?
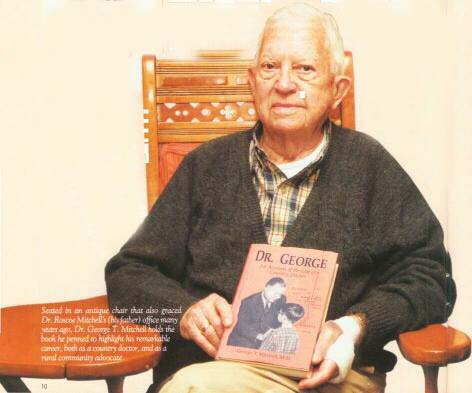
Travel back to a much simpler time when medical care consisted of a kindly man in a black overcoat visiting your home with his worn black medical bag, filled with cold steel instruments, herbs and plenty of lollipops. He drove his shiny black Ford (the only one in your small town at the time), and spent more time at patients' homes than at his office. He may have come to your home to treat your chicken pox or sniffles, or he may have even been delivering your baby sister. Because you were miles from the nearest hospital, he was rural medical care to you and your neighbors. Changing rural demographics, insurance costs, Illinois laws and declining pools of qualified employees have jeopardized the availability and quality of rural medical care today. While cooperation has always been the answer to many rural problems, ingenuity and technology are proving increasingly vital in ensuring that our children and grandchildren won't compromise their healthcare by living in rural America. Dr. George Mitchell of Marshall is the epitome of the doctor with the shiny Ford and worn black medical bag, and he's served patients in Clark County for nearly 60 years. He's seen medical care evolve over the years, all the while experiencing the trials and tribulations of struggling to maintain quality healthcare in his small community. Always a progressive thinker and someone who didn't believe that rural healthcare should
10 | Illinois Country Living | www.icl.coop be sub-par to urban healthcare, Mitchell is indeed considered a healthcare pioneer. In 1968, when the 16 doctors who had been practicing in Clark County dwindled to just four, Dr. Mitchell was the only physician left to serve 6,000 to 7,000 patients throughout the eastern side of the county. Marshall townspeople, frantic to bring in another doctor, called a town meeting to discuss the problem. Dr. Mitchell knew that Marshall couldn't compete with neighboring hospitals to attract a young doctor to the area, so during the town meeting, he brought up the novel idea of a medical center. Such a center would group a number of doctors together, and the facility would include laboratories, physical therapy and emergency services; things that none of the doctors could afford to fund alone - a cooperative of sorts. One medical center would be located in Marshall and another on the opposite side of the county in Casey, both attached to existing nursing homes. The Marshall townspeople immediately embraced the medical center concept, and Mitchell took the idea to the Illinois State Medical Society, who financed a consultant to conduct a feasibility study. The consultant, intrigued with the concept, gave them the green light, and the race to raise necessary funds began immediately. Dr. Mitchell says that neither medical center was financed by government or state money. It was the community that stepped up to the challenge, with its citizens bankrolling the $550,000 required for each medical center. The kids even got caught up in the excitement, donating their allowances and selling candy to support the idea. Dr. Mitchell says, "If you are going to draw doctors, you must have something like this to attract them. Today's solo practitioners are coming right out of medical school, and they've got maybe a $100,000 debt before they even start practicing. To just be starting out and have to invest in equipment and pay office rental is simply not that attractive." He said the idea was to put doctors together in one building so they could cover each other's appointments when necessary, share expenses, and have partners with whom to consult.
When the new medical centers opened, Marshall was besieged with people who wanted a glimpse of this revolutionary idea. Dr. Mitchell recalls, "We had people from as far away as North Carolina coming to see the medical centers. They said we were the first ones to give the idea a try. It was called the new concept in rural medicine." The medical centers still operate at full capacity today. Dr. Mitchell is also very committed to doing what he can to help grow the number of rural physicians in Illinois. He is actively involved in the Rural Medical Education (R-MED) program, offered through the University of Illinois College of Medicine at Rockford. The purpose of the program is to admit and prepare medical students from Illinois who plan to stay in the state as primary care physicians. The program is limited to just 48 applicants, and with the help of medical school faculty and the selection and recruitment committee, on which Dr. Mitchell serves, that number is whittled down to just 15-16 students who will enter the rural medical program, along with traditional medical students. The program offers students the opportunity to work alongside rural physicians, participate in summer internships at rural clinics, take part in rural health seminars, and gain patient experience during internships with rural hospitals or clinics. The hope is that students will like the atmosphere and return to practice there upon graduation. Mitchell says, "Statistics have shown it's been a very successful thing. Most of those students come from towns of less than 20,000 populations, and they're going back into those areas. You've got to grow your own. I've found that to be true, and I've known it all along." Physician vacancies aren't the only healthcare positions that are becoming increasingly difficult to fill. With an ever-decreasing pool of qualified service employees, it's a fight for rural healthcare facilities to draw the workers necessary March 2004 | www.aiec.coop | 13
And service employees have more alternatives than ever from which to choose. Barbara Bock Dallas, Senior Director of the Illinois Hospital Association, agrees, "Rural people are really scrutinizing these new possibilities. With more glamorous employers, such as riverboats, moving in, medical facilities have to fight to be employers of choice." Communities must be advocates and support their local health-care providers to keep them there. Hospitals are often the largest employers in the town, or even in the county, employing 22 percent of the rural population, so it's vital to keep them there. Dallas says if you pick up on a rumor that someone got bad emergency room care, you can't just turn around and tell that to the next person. Even one malicious rumor can do irreversible damage to a facility. She advises, "You need to call the hospital administrator and tell him what you're hearing. And get straight answers. This is your hospital and you want to keep it there. Just like everything else, if you don't use those rural providers, you'll lose them."
With the number of medical facilities on the decline, the healthcare industry will be scrambling to accommodate the growing number of baby boomers. Representing a whopping 30 percent of our population, baby boomers are now skating close to retirement, and will soon begin experiencing increased health issues. Sheldon Keyser, recent retiree of the United States Department of Agriculture Rural Development, says, "Something like 80 percent of your health costs are incurred after age 65." That, coupled with the fact that nearly 25 percent of rural America is uninsured, will not only flood medical facilities, but those facilities will see a growing percentage of uncollectible accounts and accounts receivable. Often when patients are uninsured, they cannot afford to pay for healthcare. Hospitals are mandated to accept any patient who is referred by a physician. If the medical facility can't collect the medical bill from the patient, it must pass those costs to wherever it can. Unfortunately, that could be to you. Emergency services, which have also been disappearing from many communities, will he necessary to serve our aging population. Most emergency services are supported by the local tax base, and in a number of rural counties, especially in southern Illinois, the tax base is decreasing. That means the affected medical facilities must cut 12 | ILLINOIS COUNTRY LIVING | www.icl.coop back on emergency services and training, replacing equipment, or worse yet, be forced to close altogether. Keyser recalls, "I know of one county in Illinois where their ambulance broke down, and they were driving a personal vehicle that didn't even have the necessary equipment for transporting patients. It's better than nothing, but not much." Probably the most difficult hurdle to overcome in medical costs and medical care is the dirty little "m" word — malpractice insurance for liability litigation. According to Keyser, medical malpractice insurance premiums have increased in Illinois dramatically, forcing physicians to relocate their practices to other states. By relocating, some physicians are seeing a drop in their malpractice insurance premiums by as much as $100,000 per year. The remaining Illinois doctors have been forced to raise their fees to cover the cost of the insurance, and/or see more patients per hour to make up the difference. Keyser adds, "When the doctor comes in, he's in a greater hurry, talks to me less, gives me less personal attention, and is less likely to ask critical questions." Even Dr. Mitchell is carrying the burden of rising malpractice insurance costs. He says he sees only a minimal number of patients per day and pays the lowest malpractice insurance rates available. "I'm working part time here, so I get a special rate on my malpractice insurance. But, it still costs me $14,000 per year. If you consider that, along with the other expenses I have, I'm not making a dime on the practice of medicine. In fact, I'm subsidizing it." Dallas says the malpractice insurance issue is being argued at the federal level, and she believes it's the only way it will ever be settled. According to her, Illinois is at the top of a list of states where malpractice insurance rates are out of control. So, how do we solve the problem of reduced medical services for whatever reason? One answer is telemedicine. Through telemedicine, fewer doctors and nurses will be necessary, we'll need fewer healthcare facilities, and medical costs on the whole should decrease. Soon all telephone lines will be able to accommodate high-speed data transfer, enabling patients to receive services such as medical consultations, follow-ups and surgical procedures — thus allowing anyone, regardless of where they live, to receive superior health care. And some patients with high speed Internet access are already able to receive the benefits of telemedicine without leaving their homes. For example, a patient who is recovering from heart surgery could forego driving to the healthcare facility for a check-up. A remote blood pressure cuff and heart monitor hooked into a computer modem at his home could send instantaneous reports to a doctor in an office many miles away, who could evaluate the reports and ask the patient questions accordingly. Dr. Mitchell is a strong advocate of telemedicine. For one thing, the idea of elderly patients getting out on the highway and traveling sometimes a long distance to the nearest healthcare facility concerns him. He says, "I've envisioned having telecommunication between our local clinics in Marshall and Casey, and Union Hospital and all the specialists in Terre Haute. We'd be connected to the specialists, so if we have a patient here with a problem, instead of sending them over there, we could instantaneously treat them by telemedicine. The more isolated the place is, the more important that you'd need technology like that." And, even surgery is being performed remotely using robotics, and virtual instruction for procedures can occur between a medical facility here and one overseas. The possibilities are endless. Although there may be a shadow over the healthcare industry now, Mitchell, Dallas and Keyser look to the future somewhat optimistically. They believe that if a community is willing to work cooperatively, look at the necessary technology and be open to innovative ideas, rural healthcare can he resuscitated. They also agree that rural healthcare is simply "neighbors helping neighbors." Maybe rural healthcare isn't exactly what it was in the past; but somehow, some way, a doctor will always be in the house, and through technology, maybe even on a computer screen in your house.
March 2004 | www.aiec.coop | 13 |
|
|